What Is Thyroid Eye Disease (TED)?
Thyroid Eye Disease (TED), also called Graves ophthalmopathy or thyroid-associated ophthalmopathy, is an autoimmune condition affecting the tissues around and behind the eyes.
The condition involves inflammation of the muscles, fat and connective tissue inside the eye socket (orbit). This swelling pushes the eyeballs forward, causing the characteristic bulging appearance.
TED most commonly occurs in people with Graves disease, but it can also occur in people with Hashimoto’s thyroiditis or even in people whose thyroid hormone levels are normal.
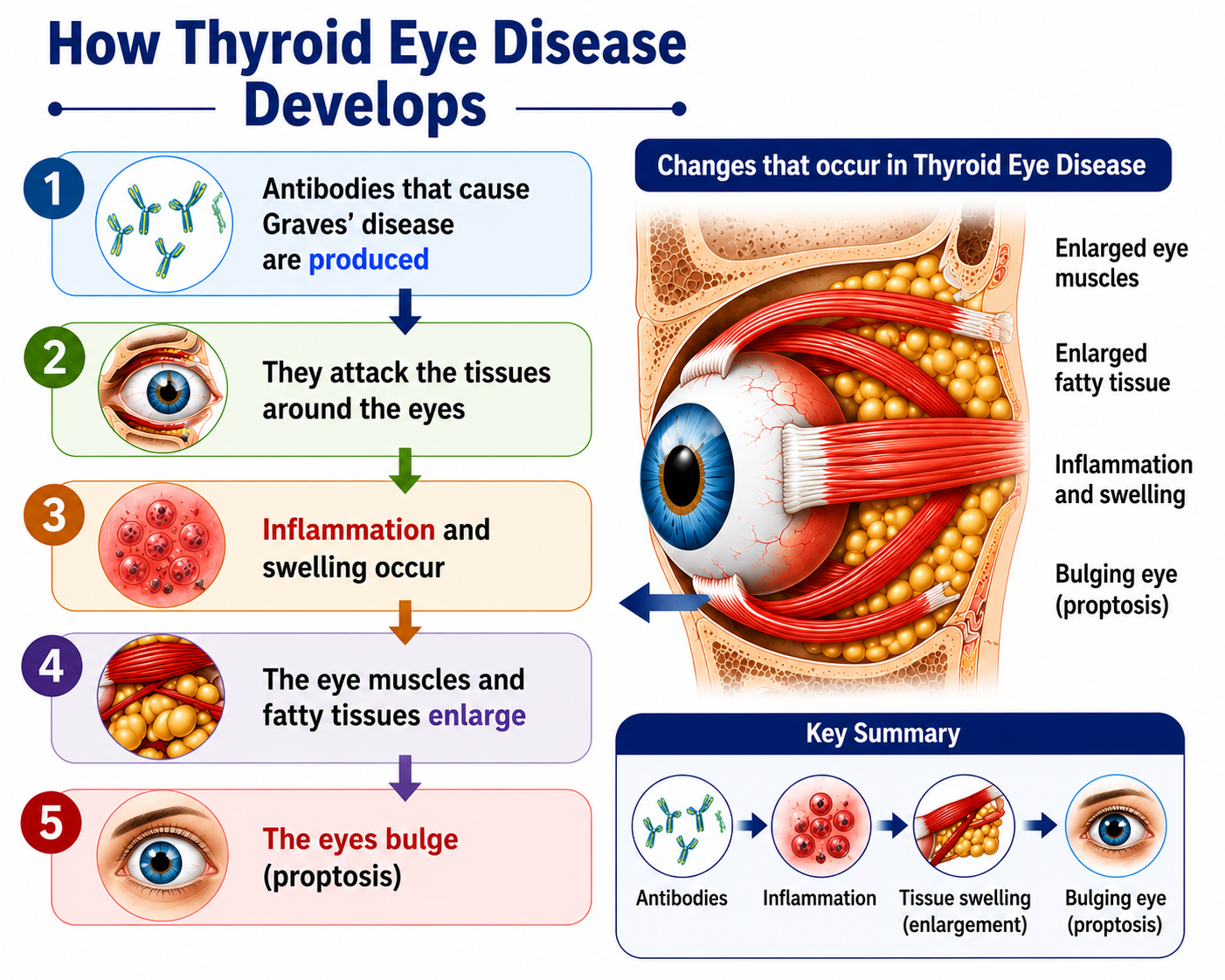
How Does Thyroid Eye Disease Develop?
The same antibodies responsible for Graves disease — TSH receptor antibodies (TRAb) — also target the connective tissue and fat cells inside the eye socket.
In the orbit, these antibodies stimulate cells in the tissues behind the eyes. These cells produce substances that attract water, causing swelling of the muscles, fat and connective tissue inside the eye socket.
The result is increased volume of tissue inside the fixed bony eye socket, which forces the eyeball to push forward.
Why Can TED Occur Even When Thyroid Levels Are Normal?
The orbital inflammation in TED is driven by the autoimmune process itself, not directly by thyroid hormone levels. This is why TED can appear before hyperthyroidism is diagnosed, persist after thyroid levels are normalised, or occasionally develop in people who have never had abnormal thyroid function.
Can Thyroid Eye Disease Occur Without Hyperthyroidism?
Yes. Although Thyroid Eye Disease most commonly occurs in people with Graves disease and hyperthyroidism, it can occasionally occur when thyroid hormone levels are normal.
In some people, eye symptoms appear before thyroid blood tests become abnormal. In others, the eye disease may continue even after thyroid hormone levels are brought under control.
Does Everyone With Graves Disease Develop Thyroid Eye Disease?
No. Not everyone with Graves disease develops Thyroid Eye Disease.
Many people with Graves disease never develop significant eye involvement. Some develop only mild eye symptoms, while a smaller group develop moderate or severe disease.
Smoking greatly increases the chance of developing more severe Thyroid Eye Disease.
How Common Is Thyroid Eye Disease?
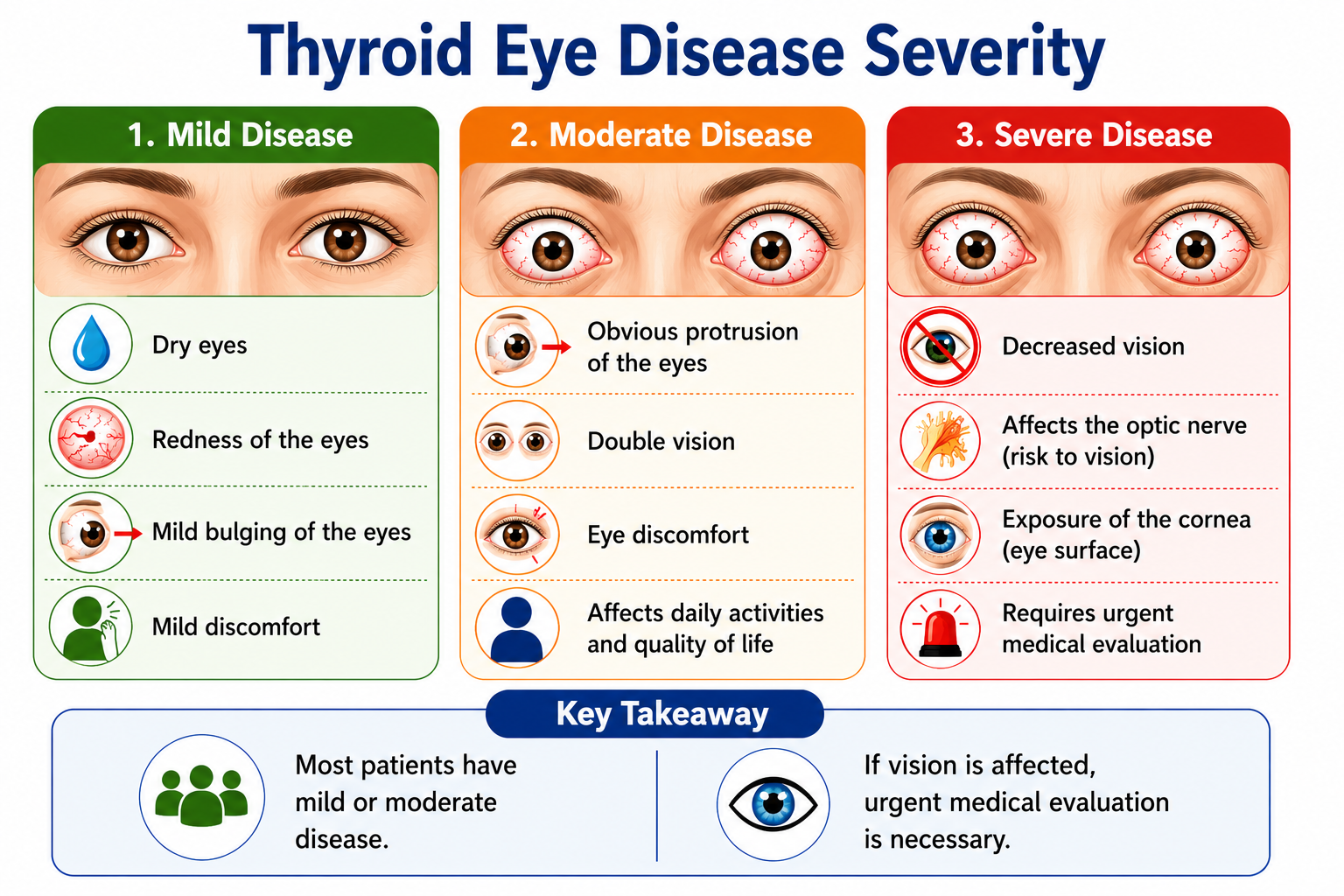
Mild eye symptoms are relatively common in people with Graves disease. However, severe or sight-threatening Thyroid Eye Disease is uncommon.
Most patients do not develop permanent vision problems, especially when the condition is recognised early and managed appropriately.
Symptoms of Thyroid Eye Disease
Symptoms vary considerably depending on the severity of the condition. Early TED often causes mild discomfort, while severe TED can threaten vision.
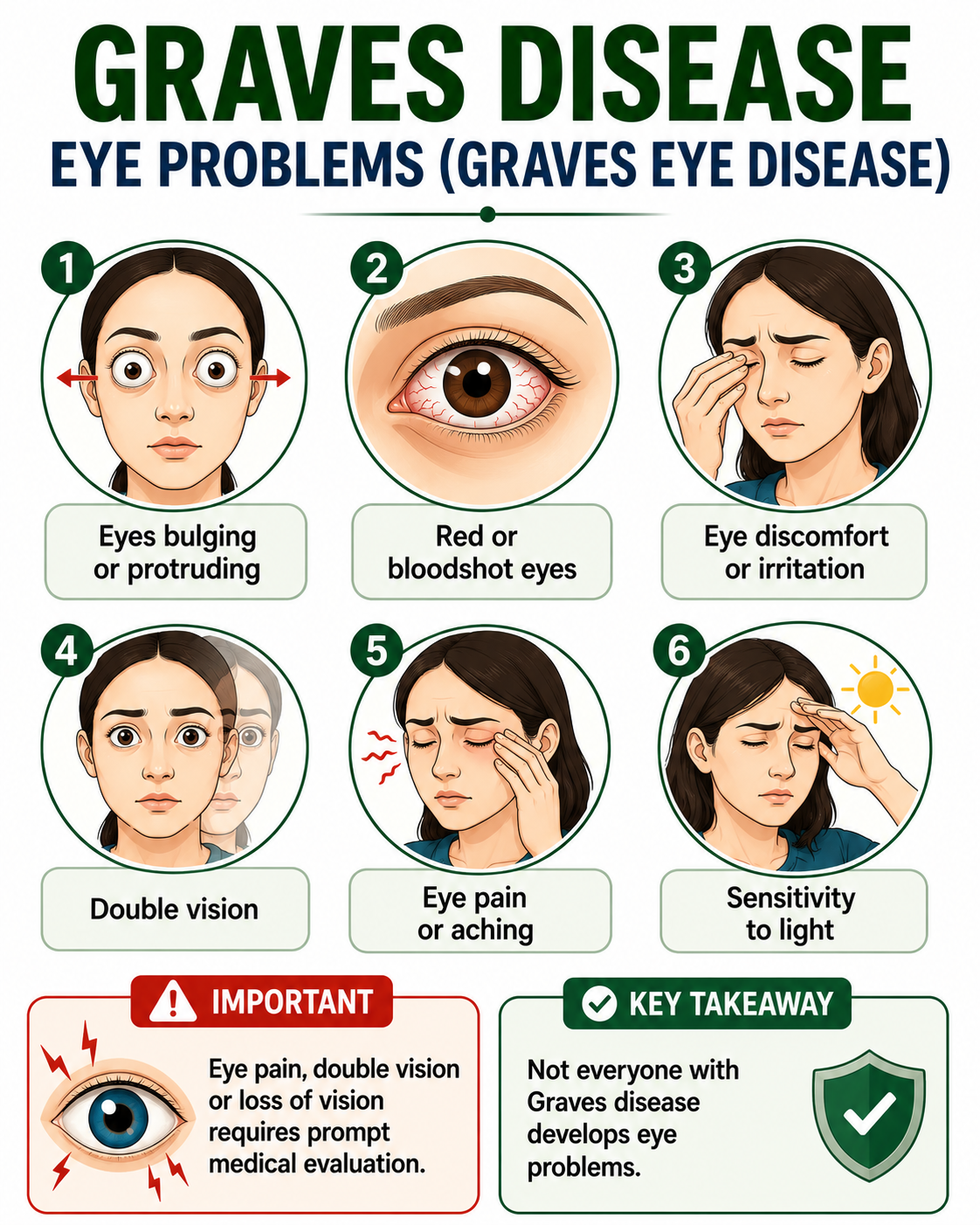
Proptosis (Bulging Eyes)
Proptosis, also called exophthalmos, is the most recognised feature of TED. The eyeballs are pushed forward because the swollen orbital tissues have no room to expand within the rigid bony eye socket.
Proptosis may affect one or both eyes and may be asymmetric.
Eyelid Changes
The upper eyelids may retract, making the eyes appear wide and staring. In severe cases, the eyelids may not close fully during sleep, leading to corneal exposure and dryness.
Double Vision
Swelling and inflammation of the eye muscles can cause them to become stiff and poorly coordinated. This restricts eye movement and produces double vision (diplopia), which may be worse in certain gaze positions.
Severity of Thyroid Eye Disease
TED ranges from mild to sight-threatening. Clinicians assess both the severity of structural changes and the activity of the inflammatory process.
| Severity Grade | Typical Features |
|---|---|
| Mild | Minor eyelid retraction, mild soft tissue involvement, no or minimal proptosis, no double vision, corneal exposure controllable with lubricants |
| Moderate to Severe | Significant eyelid retraction, moderate to severe soft tissue involvement, proptosis, double vision, corneal exposure not fully controlled with lubricants |
| Sight-Threatening | Dysthyroid optic neuropathy (optic nerve compression) causing reduced or colour vision, or severe corneal breakdown |
Active vs Inactive TED
TED has two phases. During the active (inflammatory) phase, the condition is progressing and the tissues are acutely inflamed. During the inactive (chronic) phase, inflammation has settled but structural changes may persist.
The Clinical Activity Score (CAS) is used to assess whether TED is in the active phase. This distinction guides treatment decisions because immunosuppressive treatments are most effective during the active phase.
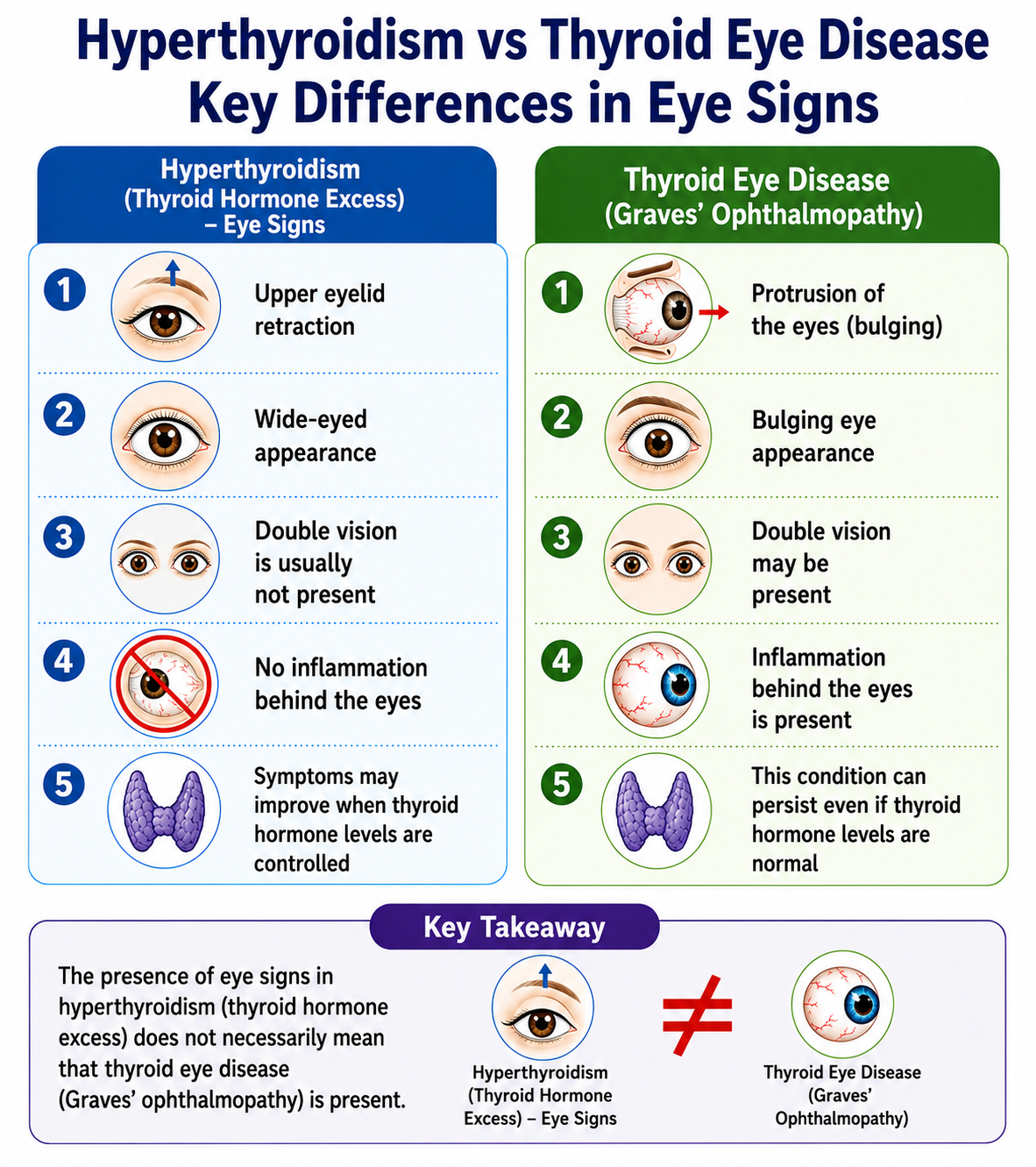
Hyperthyroidism Eye Signs vs Thyroid Eye Disease
Many people assume that all eye symptoms in hyperthyroidism are caused by Thyroid Eye Disease. This is not always true.
Hyperthyroidism itself can cause changes in eyelid position and eye appearance due to excess sympathetic nervous system activity. These are different from the orbital inflammation of TED.
| Hyperthyroidism Eye Signs | Thyroid Eye Disease |
|---|---|
| Eyelid retraction | True eye protrusion (proptosis) |
| Staring appearance | Bulging eyes |
| Usually no double vision | Double vision possible |
| No orbital inflammation | Orbital inflammation present |
| Often improves with thyroid control | May persist despite normal thyroid tests |
Not every patient with hyperthyroidism has Thyroid Eye Disease, and not every patient with Thyroid Eye Disease develops severe eye protrusion.
Who Is at Risk of Thyroid Eye Disease?
Not all people with Graves disease develop TED. Several factors influence the risk:
- Graves disease — the strongest risk factor; most TED patients have Graves disease
- Smoking — significantly increases the risk and severity of TED
- Female sex — TED is more common in women, though men who develop it tend to have more severe disease
- Age — risk increases with age and older patients may have more severe TED
- Radioactive iodine treatment — may worsen or trigger TED in some patients with pre-existing eye disease or high TRAb levels
- Poorly controlled thyroid levels — unstable thyroid hormone levels may influence TED activity
- High TRAb levels — elevated TSH receptor antibody levels are associated with a greater risk of significant TED
Smoking and Thyroid Eye Disease
Smoking is the single most important modifiable risk factor for Thyroid Eye Disease.
People who smoke are significantly more likely to develop TED, more likely to develop severe TED, and less likely to respond well to immunosuppressive treatment.
Stopping smoking reduces the risk of developing TED, may slow its progression, and improves the likelihood of a good response to treatment. The benefit of stopping smoking is seen even in people who already have TED.
How Is Thyroid Eye Disease Diagnosed?
Diagnosis is based on clinical examination of the eyes together with thyroid blood tests. In most cases the combination of typical eye findings and Graves disease makes the diagnosis clear.
Blood Tests
| Test | Relevance in TED |
|---|---|
| TSH | Usually low in active Graves disease; may be normal in some TED patients |
| Free T4 / Free T3 | Elevated in active hyperthyroidism; may be normal |
| TRAb | Usually Positive — helps confirm the autoimmune basis of TED |
Eye Assessment
Assessment by an ophthalmologist is recommended for significant TED. This includes measurement of proptosis, assessment of eye muscle function, visual acuity, colour vision, optic nerve evaluation and Clinical Activity Score (CAS).
Orbital Imaging
CT or MRI of the orbits may be needed to assess the degree of muscle swelling, orbital tissue volume and proximity of swelling to the optic nerve. Imaging guides decisions about surgical decompression.
Treatment of Thyroid Eye Disease
Treatment depends on the severity and activity of the disease. Thyroid hormone levels should be kept stable, and smoking should be stopped. Treatment for the eye condition itself is separate from treatment for hyperthyroidism.
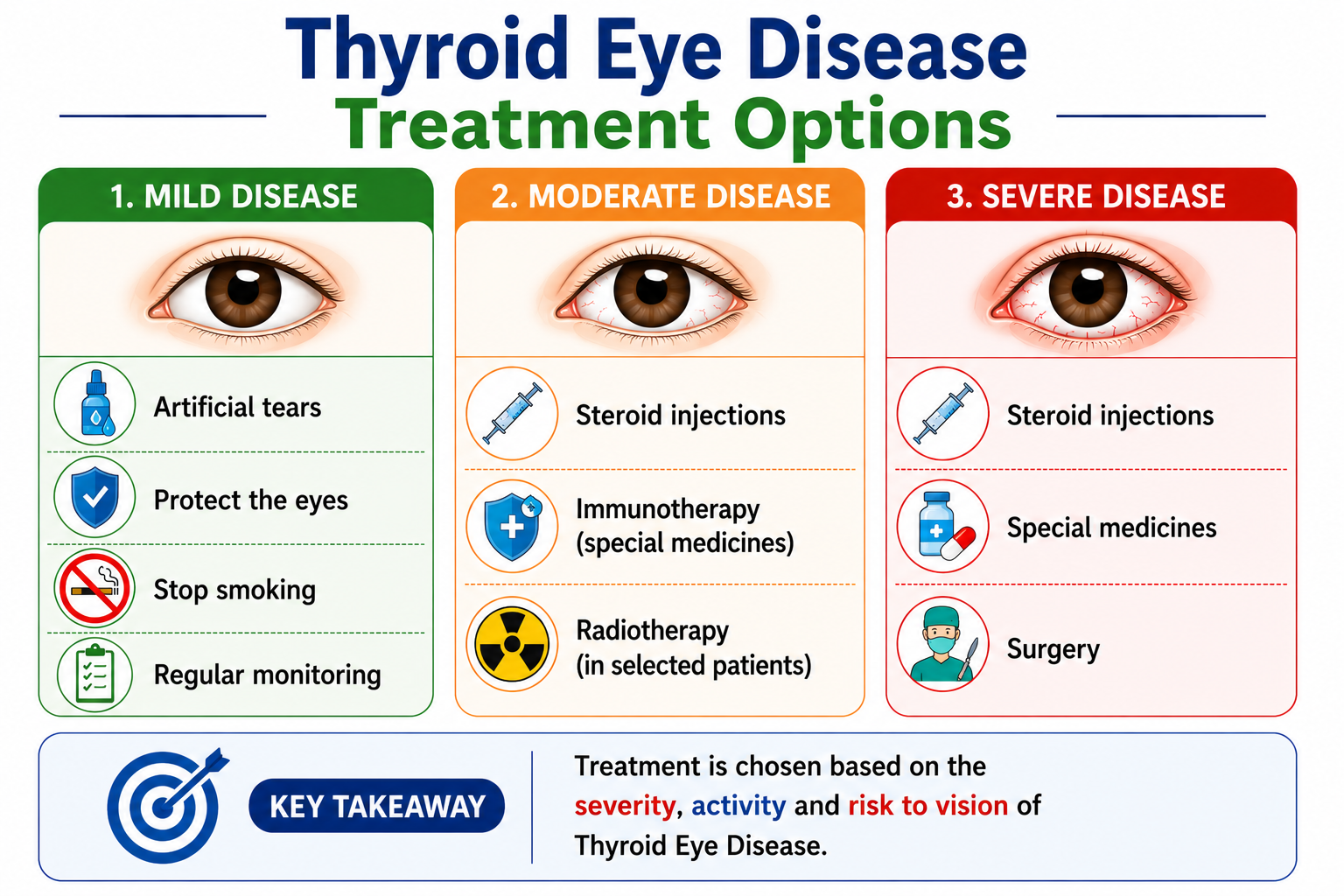
Supportive Measures
For mild TED, the focus is on symptom relief and protection of the eyes:
- Lubricating eye drops and ointments to relieve dryness and irritation
- Sunglasses to reduce light sensitivity
- Elevating the head of the bed to reduce morning eyelid swelling
- Prism glasses for double vision
Selenium Supplementation
Selenium supplementation (100 µg twice daily for 6 months) has been shown to benefit patients with mild active TED. It is not recommended for severe TED or inactive TED.
Intravenous Corticosteroids
High-dose intravenous methylprednisolone given weekly over several weeks is the main treatment for moderate-to-severe active TED. It reduces inflammation and may improve proptosis, double vision and soft tissue signs during the active phase.
Orbital Radiotherapy
Low-dose radiotherapy to the orbits may be used alongside or after corticosteroids, particularly for double vision that has not responded to steroids alone.
Biological Therapy
Teprotumumab is a targeted biological therapy approved for moderate-to-severe active TED. It blocks the IGF-1R receptor on orbital fibroblasts and has shown significant reductions in proptosis and double vision in clinical trials.
Surgery
Surgery is typically reserved for the inactive phase of TED, once inflammation has settled. Surgical options include:
- Orbital decompression — removes bone or fat from around the eye socket to reduce proptosis and relieve optic nerve pressure
- Eye muscle surgery (squint surgery) — corrects persistent double vision due to muscle fibrosis
- Eyelid surgery — corrects eyelid retraction or incomplete eyelid closure
Surgery is usually performed in this sequence: decompression first, then muscle surgery, then eyelid surgery — as each procedure can affect the others.
Emergency Warning Signs
Most cases of TED progress slowly. However, certain features indicate sight-threatening disease requiring urgent specialist assessment.
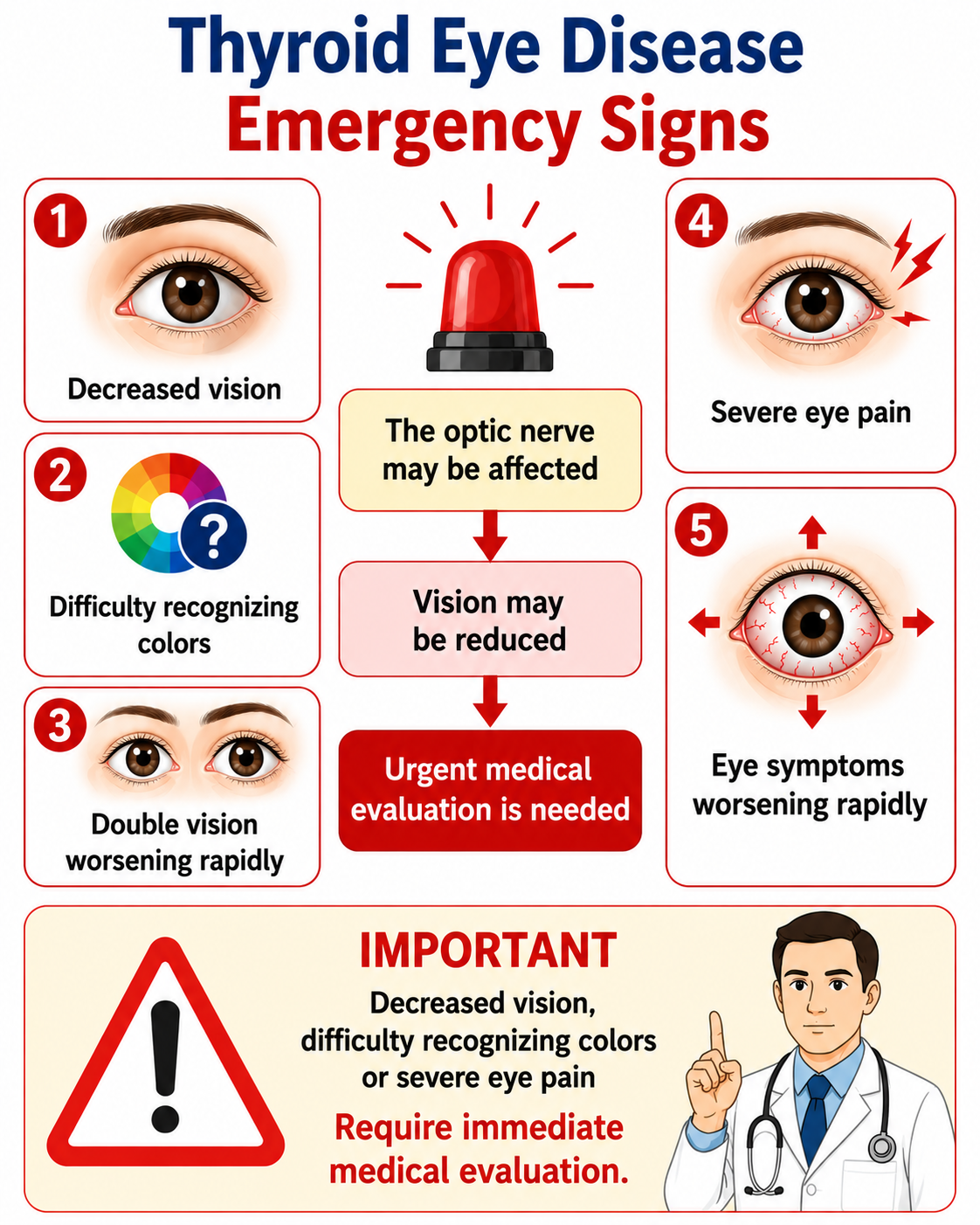
- Sudden or rapidly worsening loss of vision
- Change in colour vision (colours appear washed out or different)
- Inability to fully close one or both eyes
- Severe eye pain or pain on eye movement
- Rapidly increasing proptosis over days or weeks
Dysthyroid Optic Neuropathy
Compression of the optic nerve by swollen orbital muscles is called dysthyroid optic neuropathy (DON). It can cause colour vision changes, blurring and ultimately irreversible vision loss if untreated. DON is a medical emergency and usually requires urgent high-dose corticosteroids or emergency surgical decompression.
Corneal Exposure
If proptosis is severe enough that the eyelids cannot close properly, the cornea (front surface of the eye) becomes exposed. This can lead to corneal ulceration and vision loss. Intensive lubricating treatment, taping the eye shut at night, or urgent surgery may be needed.
Prognosis and Long-Term Outlook
The natural course of TED follows a pattern described by Rundle’s curve: gradual worsening during the active inflammatory phase, followed by a plateau and then partial spontaneous improvement.
However, structural changes such as significant proptosis, restricted eye movement and eyelid retraction often do not fully resolve without intervention.
- Mild TED frequently stabilises without significant visual impairment
- Moderate-to-severe TED may require treatment during the active phase to limit long-term structural damage
- Surgical rehabilitation in the inactive phase can significantly improve the appearance of the eyes and quality of life
- Sight-threatening TED, if treated promptly, usually has a good visual outcome
