
| TSH Result | Possible Meaning | What to Check Next |
|---|---|---|
| High TSH | Thyroid may be underactive | Free T4, symptoms, thyroid antibodies |
| Normal TSH | Thyroid function is usually normal | Review symptoms and other possible causes |
| Low TSH | Thyroid may be overactive | Free T4, Free T3, clinical assessment |
This is a simplified guide. Always interpret TSH together with your symptoms, Free T4 / Free T3 results, medicines, pregnancy status, and your laboratory reference range.
What is TSH?
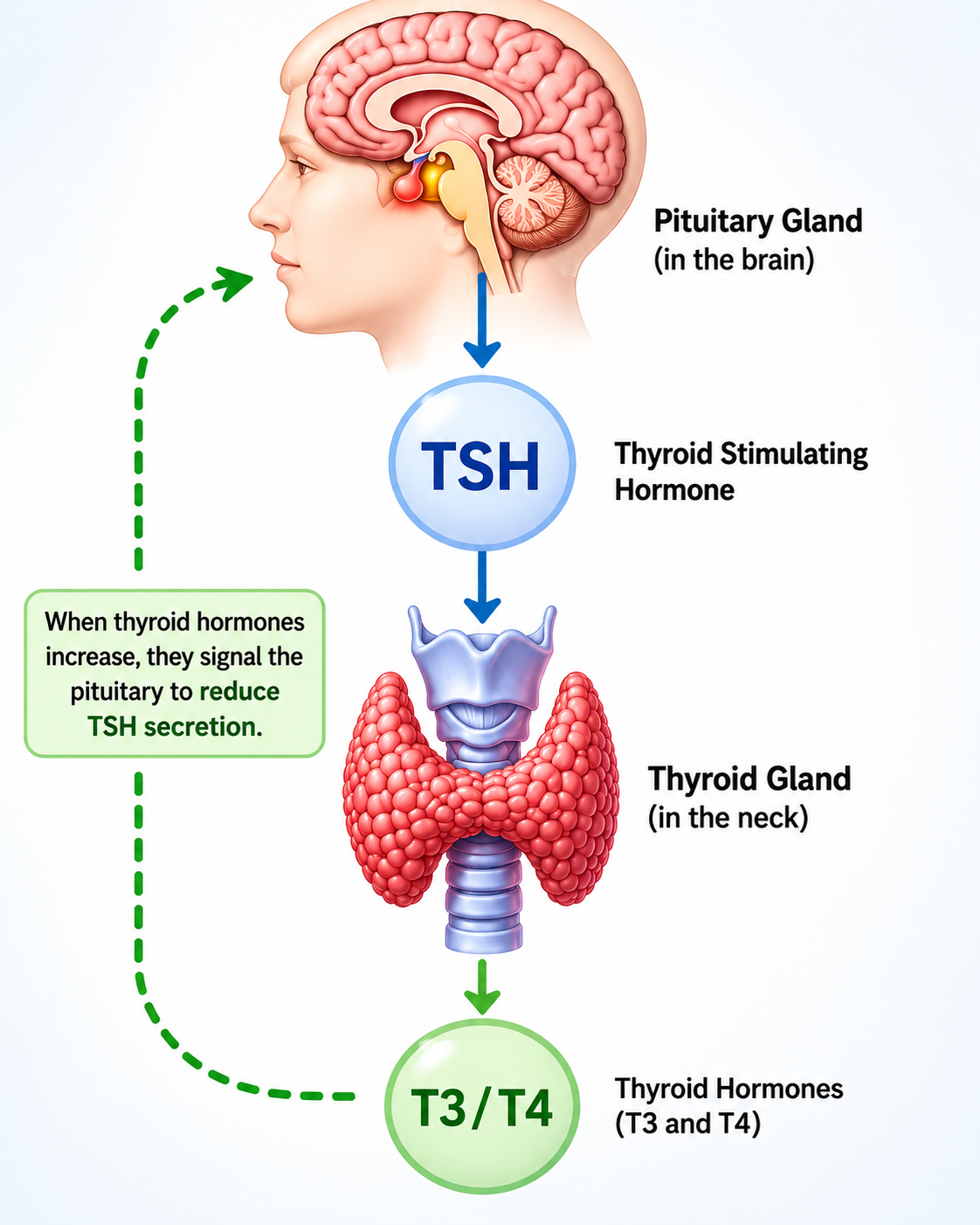
TSH stands for Thyroid Stimulating Hormone. Despite its name, TSH is not produced by the thyroid gland — it is produced by the pituitary gland, a small gland at the base of the brain approximately the size of a pea.
The pituitary gland acts as the control centre for the thyroid. It constantly monitors the amount of thyroid hormone circulating in the blood and uses TSH as a chemical signal to instruct the thyroid gland to produce more or less hormone.
When the thyroid gland responds appropriately, thyroid hormone levels rise, and the pituitary reduces its TSH output. When the thyroid fails to respond, TSH keeps rising in an attempt to stimulate it harder. This makes TSH one of the most sensitive early indicators of thyroid dysfunction — it often changes before thyroid hormone levels themselves become abnormal.
Why Do Doctors Request a TSH Test?
Doctors may request a TSH test when patients have symptoms suggesting thyroid disease. Common symptoms that prompt TSH testing include:
TSH testing is also requested routinely in the following situations:
- Monitoring patients already diagnosed with hypothyroidism or hyperthyroidism
- Checking response to thyroid replacement medication (levothyroxine)
- Screening pregnant women (thyroid problems are common in pregnancy)
- Investigating unexplained infertility or recurrent miscarriage
- Screening patients with a family history of thyroid disease
- Evaluating mood disorders, depression, or unexplained cognitive changes
How TSH Controls the Thyroid
The pituitary gland continuously monitors thyroid hormone levels in the bloodstream. This creates a self-regulating feedback loop — one of the most elegant control systems in the human body.
When thyroid hormone levels fall too low, the pituitary acts immediately:
When thyroid hormone levels are already too high, the reverse happens — the pituitary suppresses TSH production, removing the stimulus for further thyroid hormone release.
What is the Normal TSH Range?
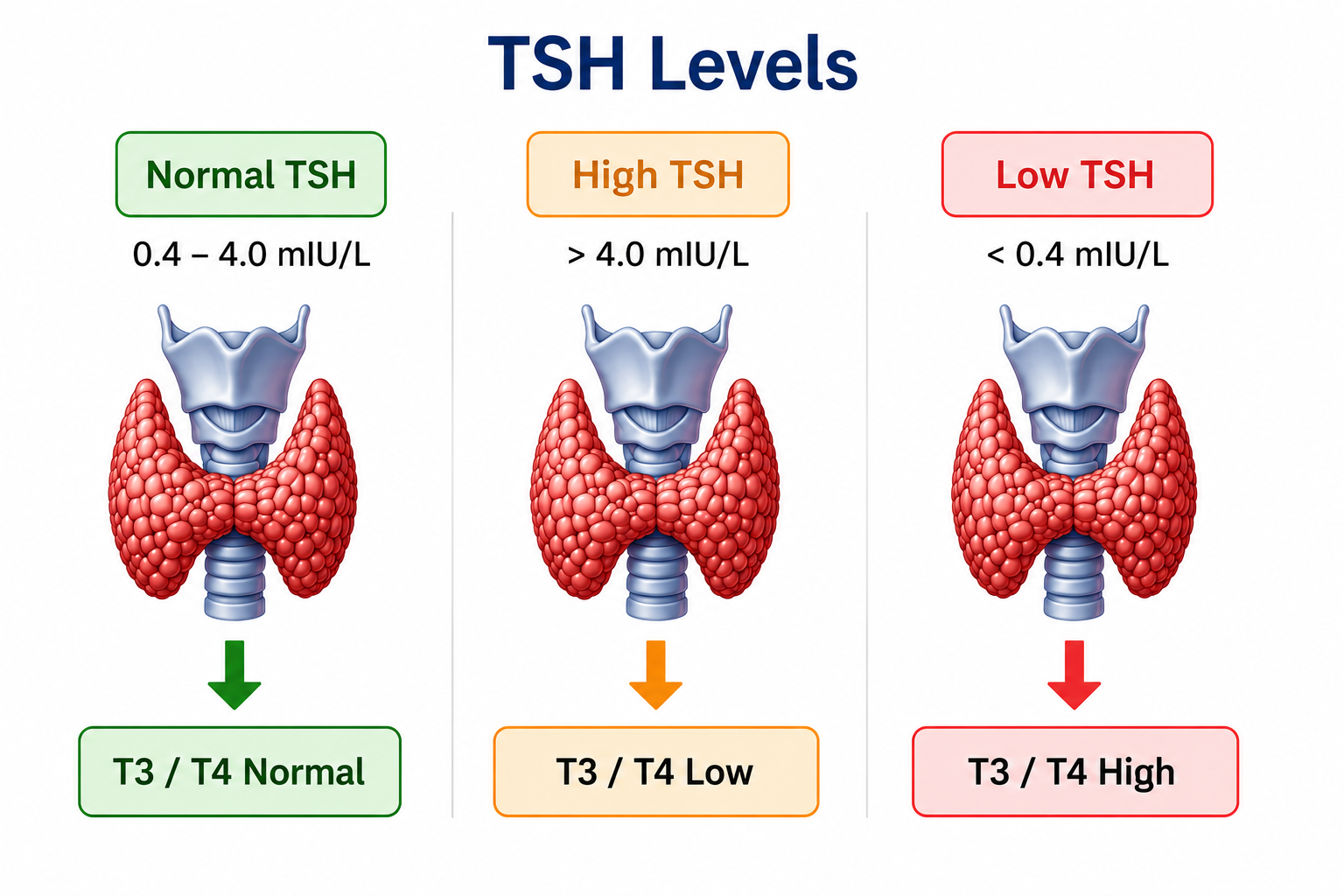
Normal ranges vary slightly between laboratories, depending on the equipment and reagents used. Most laboratories use an approximate reference range of:
0.4 – 4.0 mIU/L
Always refer to the reference range printed on your own laboratory report.
How Doctors Interpret TSH Levels
| Category | TSH Level (approx.) | What it May Suggest |
|---|---|---|
| Normal | 0.4 – 4.0 mIU/L | Thyroid function is likely normal |
| Mildly Elevated | 4.0 – 10.0 mIU/L | Possible subclinical hypothyroidism — monitoring or treatment may be considered |
| Significantly Elevated | >10 mIU/L | Hypothyroidism likely — Free T4 and clinical assessment needed |
| Low | 0.1 – 0.4 mIU/L | Borderline — subclinical hyperthyroidism possible; repeat and further testing needed |
| Suppressed | <0.1 mIU/L | Hyperthyroidism likely, or overtreatment with thyroid medication |
TSH Alone Is Not a Complete Diagnosis
TSH is the most useful first test for thyroid function, but it is not the only test doctors use. A TSH result should always be interpreted together with symptoms, examination findings, other thyroid hormone levels, medicines, pregnancy status, and the laboratory reference range.
In many cases, doctors request additional tests before confirming a diagnosis or starting treatment.
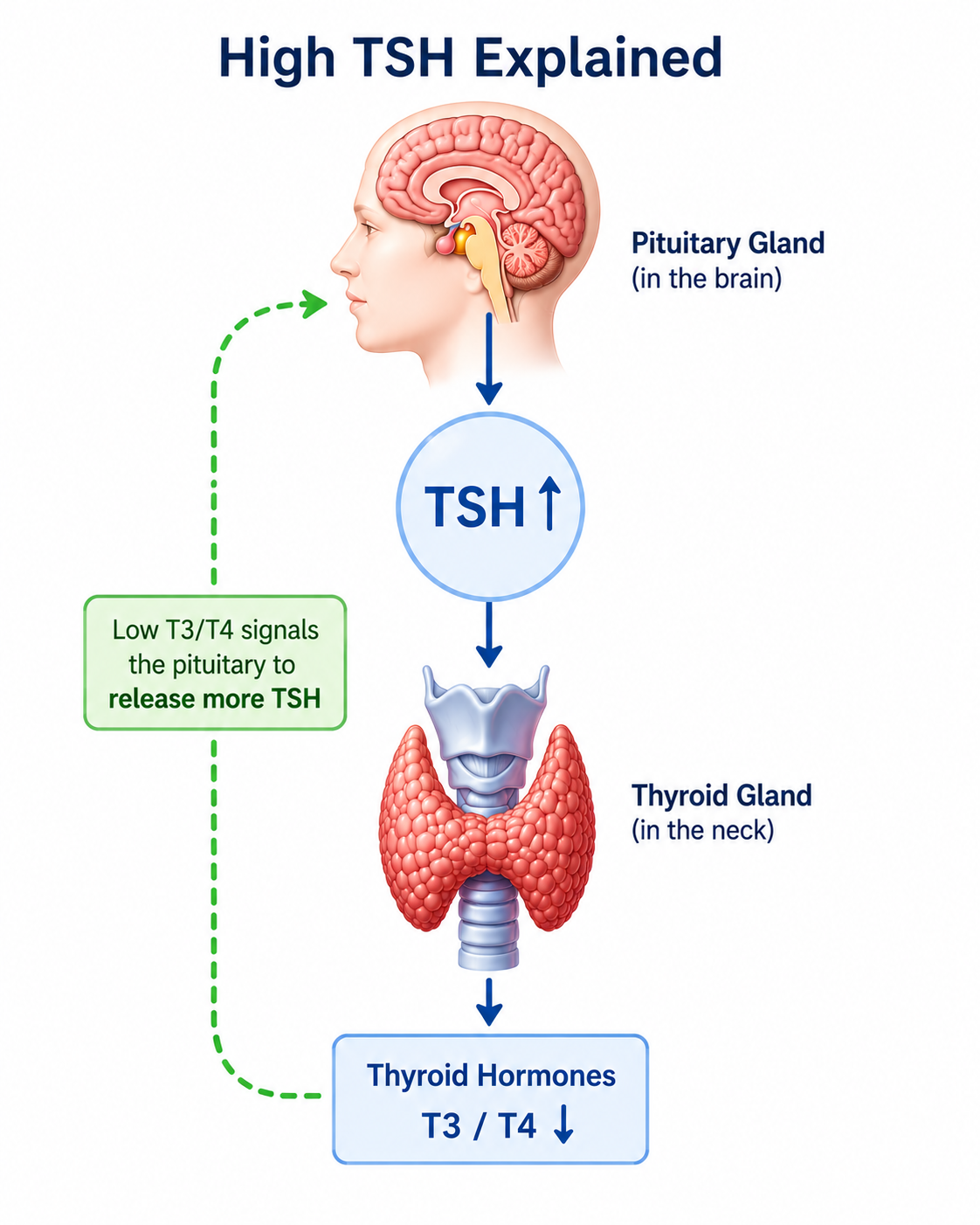
What Does a High TSH Mean?
A high TSH usually suggests that the thyroid gland is not producing enough thyroid hormone. The pituitary gland detects low T4 in the blood and responds by releasing more and more TSH — essentially working harder to push a failing thyroid.
Common Causes of High TSH
- Primary hypothyroidism — the thyroid gland itself is underperforming (most common cause)
- Hashimoto's thyroiditis — autoimmune destruction of thyroid tissue
- Post-thyroid surgery — partial or total removal of the thyroid gland
- Radioactive iodine treatment — used for hyperthyroidism or thyroid cancer
- Certain medications — lithium, amiodarone, some immunotherapy drugs
- Subclinical hypothyroidism — TSH mildly elevated but Free T4 still normal
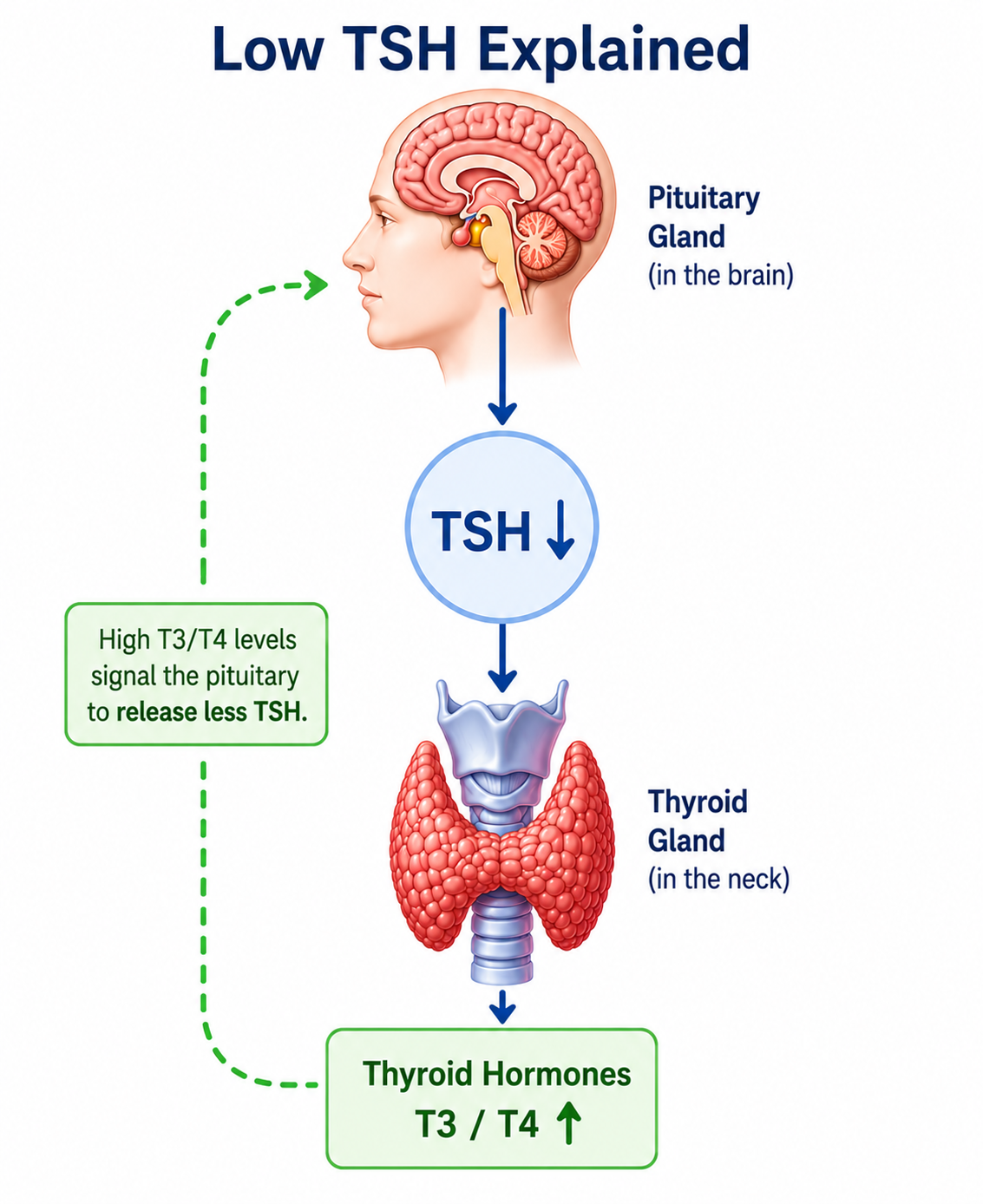
What Does a Low TSH Mean?
A low TSH usually suggests that the thyroid is producing excessive amounts of thyroid hormone. The pituitary senses that T4 and T3 are already too high and reduces its TSH output — removing the stimulus for further thyroid hormone release.
Common Causes of Low or Suppressed TSH
- Graves' disease — the most common cause of primary hyperthyroidism
- Toxic nodular goitre — overactive thyroid nodule(s) producing excess hormone
- Overtreatment with levothyroxine — dose too high for the patient's needs
- Thyroiditis — inflammation releasing stored thyroid hormone
- Subclinical hyperthyroidism — TSH low but Free T3/T4 still in range
- Excess iodine intake — through medications or supplements
Examples of TSH Result Interpretation
The meaning of TSH becomes clearer when it is interpreted together with Free T4 and symptoms.
| Example Result | Possible Interpretation | Usual Next Step |
|---|---|---|
| TSH 12 mIU/L + Free T4 low | Likely overt hypothyroidism | Medical review and treatment planning |
| TSH 6 mIU/L + Free T4 normal | Possible subclinical hypothyroidism | Repeat test, symptoms, antibodies, risk factors |
| TSH 0.02 mIU/L + Free T4 high | Likely overt hyperthyroidism | Urgent medical review and further thyroid tests |
| TSH 0.2 mIU/L + Free T4 normal | Possible subclinical hyperthyroidism | Repeat test and assess symptoms / medicines |
| TSH normal + persistent symptoms | Thyroid disease less likely, but not impossible | Review Free T4, Free T3, other causes |
Can TSH Be Normal Even When Thyroid Disease Exists?
Yes — there are important situations where a normal TSH does not rule out thyroid disease:
Early Thyroid Disease
In the very early stages, the feedback system may still be able to compensate. TSH may be at the upper or lower limit of normal while the thyroid is already beginning to fail or overperform. Serial monitoring over time can reveal a trend before levels cross the reference range cutoff.
Central Hypothyroidism
If the problem lies in the pituitary gland itself (rather than the thyroid), the pituitary may fail to produce adequate TSH even when thyroid hormone levels are low. This is called central or secondary hypothyroidism. In this rare condition, TSH may be low or inappropriately "normal" despite the patient being hypothyroid. Free T4 testing is essential in this situation.
Laboratory and Timing Variation
TSH can fluctuate throughout the day — it is naturally higher in the early hours of the morning and lower in the afternoon. For consistency, most laboratories prefer morning samples. A single borderline result should always be interpreted cautiously, and may need to be repeated.
Can Stress, Illness, or Medications Affect TSH?
Several external factors can affect TSH readings, sometimes producing results that do not reflect the true underlying thyroid status:
Non-Thyroidal Illness Syndrome
Severe acute illness — such as a serious infection, major surgery, or critical illness — can temporarily suppress TSH and alter T3 and T4 levels even when the thyroid gland is perfectly normal. This is sometimes called "sick euthyroid syndrome." TSH tested during a period of acute illness should generally be repeated after recovery before any thyroid diagnosis is made.
Medications That Affect TSH
- High-dose biotin (Vitamin B7) — can falsely suppress TSH in laboratory assays; stop biotin supplements at least 48–72 hours before testing
- High-dose corticosteroids (steroids) — can suppress TSH temporarily
- Dopamine and dopamine agonists — used in ICU settings; suppress TSH
- Amiodarone — heart medication that can cause both hypothyroidism and hyperthyroidism, and alters TSH directly
- Lithium — commonly used in bipolar disorder; can cause hypothyroidism and raise TSH
TSH During Pregnancy
Pregnancy requires special thyroid monitoring because thyroid hormones are critical for healthy fetal brain development — especially during the first trimester, when the fetus cannot yet produce its own.
Different Reference Ranges in Pregnancy
TSH normal ranges in pregnancy are lower than in the general population, particularly in the first trimester. This is partly because the pregnancy hormone hCG (human chorionic gonadotropin) has a mild TSH-like stimulating effect on the thyroid, naturally lowering TSH in early pregnancy.
| Trimester | Approximate TSH Range |
|---|---|
| First trimester (0–12 weeks) | 0.1 – 2.5 mIU/L |
| Second trimester (13–26 weeks) | 0.2 – 3.0 mIU/L |
| Third trimester (27–40 weeks) | 0.3 – 3.0 mIU/L |
Ranges are approximate; your doctor will use trimester-specific values from your laboratory.
Risks of Untreated Thyroid Disease in Pregnancy
- Increased risk of miscarriage and preterm birth
- Risk of pre-eclampsia (high blood pressure in pregnancy)
- Impaired fetal brain and nervous system development
- Low birth weight
Who Should Consider TSH Testing Before Pregnancy?
TSH testing may be especially important before or early in pregnancy if there are risk factors for thyroid disease.
- Previous miscarriage or recurrent pregnancy loss
- Difficulty becoming pregnant or infertility investigation
- Known thyroid disease in the past
- Family history of thyroid disease
- Goitre, thyroid swelling, or thyroid nodules
- Symptoms such as fatigue, weight change, palpitations, or menstrual irregularity
- Use of thyroid medication such as levothyroxine
When Should TSH Be Repeated?
Repeat TSH testing is required in several situations. The timing depends on the clinical situation:
| Situation | Recommended Timing |
|---|---|
| After starting levothyroxine treatment | Repeat in 6–8 weeks |
| After a dose change | Repeat in 6–8 weeks |
| Once stable on treatment | Every 6–12 months |
| Borderline or uncertain result | Repeat in 3–6 months |
| During pregnancy (on levothyroxine) | Once per trimester minimum |
| After acute illness or hospital discharge | Repeat 4–6 weeks after recovery |
| Persistent symptoms despite normal TSH | Add Free T4 and Free T3 |
Related Thyroid Articles and Tools
This TSH guide is part of our thyroid education series. These pages can help you understand symptoms, abnormal results, and the next steps more clearly.
