ALP and GGT help doctors assess bile flow problems
ALP (alkaline phosphatase) and GGT (gamma-glutamyl transferase) are blood tests commonly included in a liver profile.
Unlike AST and ALT blood tests, which mainly reflect liver cell injury, ALP and GGT are especially useful when doctors suspect problems related to bile flow.
These tests can become abnormal in conditions such as gallstones, bile duct obstruction, cholestasis, alcohol-related liver disease and some medication-related liver problems.
However, ALP and GGT should not be interpreted as isolated numbers. Doctors usually interpret them together with bilirubin, AST, ALT, symptoms, examination findings and imaging studies such as ultrasound scans.
What are ALP and GGT?
What is ALP?
ALP stands for alkaline phosphatase. It is an enzyme found in several parts of the body including the liver, bile ducts, bone, placenta and intestine.
Because ALP is present in multiple organs, a high ALP result does not automatically mean liver disease.
What is GGT?
GGT stands for gamma-glutamyl transferase. GGT is found mainly in the liver and bile ducts.
Compared with ALP, GGT is more useful for identifying whether an abnormal result is likely coming from the liver or biliary system. Doctors often interpret ALP and GGT together rather than separately.
Normal ALP and GGT ranges
ALP and GGT reference ranges can vary between laboratories. Always compare your result with the reference range printed on your own report.
| Test | Common approximate range | Important note |
|---|---|---|
| ALP | About 40-130 U/L | Can vary with age, pregnancy and bone growth |
| GGT | Often about 10-70 U/L | Ranges vary by sex, lab method and clinical context |
Why are ALP and GGT tests done?
Doctors may request ALP and GGT tests when they suspect problems involving bile flow, the liver or bile ducts.
- Jaundice
- Gallstones
- Bile duct obstruction
- Cholestasis
- Itching with suspected liver disease
- Alcohol-related liver disease
- Medication monitoring
- Abnormal liver profile follow-up
- Upper abdominal pain
- Dark urine or pale stools
What is cholestasis?
Cholestasis means impaired, reduced or blocked bile flow.
Bile is produced by the liver and normally flows through small channels inside the liver, then through bile ducts, and finally into the intestine. When this flow becomes blocked or slowed, substances such as bilirubin and bile salts may build up in the body.
Intrahepatic and extrahepatic cholestasis
Cholestasis may occur inside the liver or outside the liver.
| Type | Where the problem is | Examples |
|---|---|---|
| Intrahepatic cholestasis | Inside the liver | Hepatitis, medications, pregnancy-related cholestasis, some chronic liver diseases |
| Extrahepatic cholestasis | Outside the liver in larger bile ducts | Gallstones, bile duct obstruction, strictures, tumors compressing bile ducts |
Symptoms that may occur with cholestasis
| Symptom | Why it may occur |
|---|---|
| Itching | Bile-related substances may accumulate in the body |
| Jaundice | Bilirubin may increase |
| Dark urine | Direct bilirubin may enter urine |
| Pale stools | Less bile reaches the intestine |
Why can cholestasis cause itching?
Persistent itching can occur in some cholestatic liver and bile duct conditions. It is thought to be related to the build-up of bile-related substances in the body when bile flow is impaired.
Itching from cholestasis can occur even before jaundice becomes obvious in some patients. It should be interpreted together with ALP, GGT, bilirubin and the clinical situation.
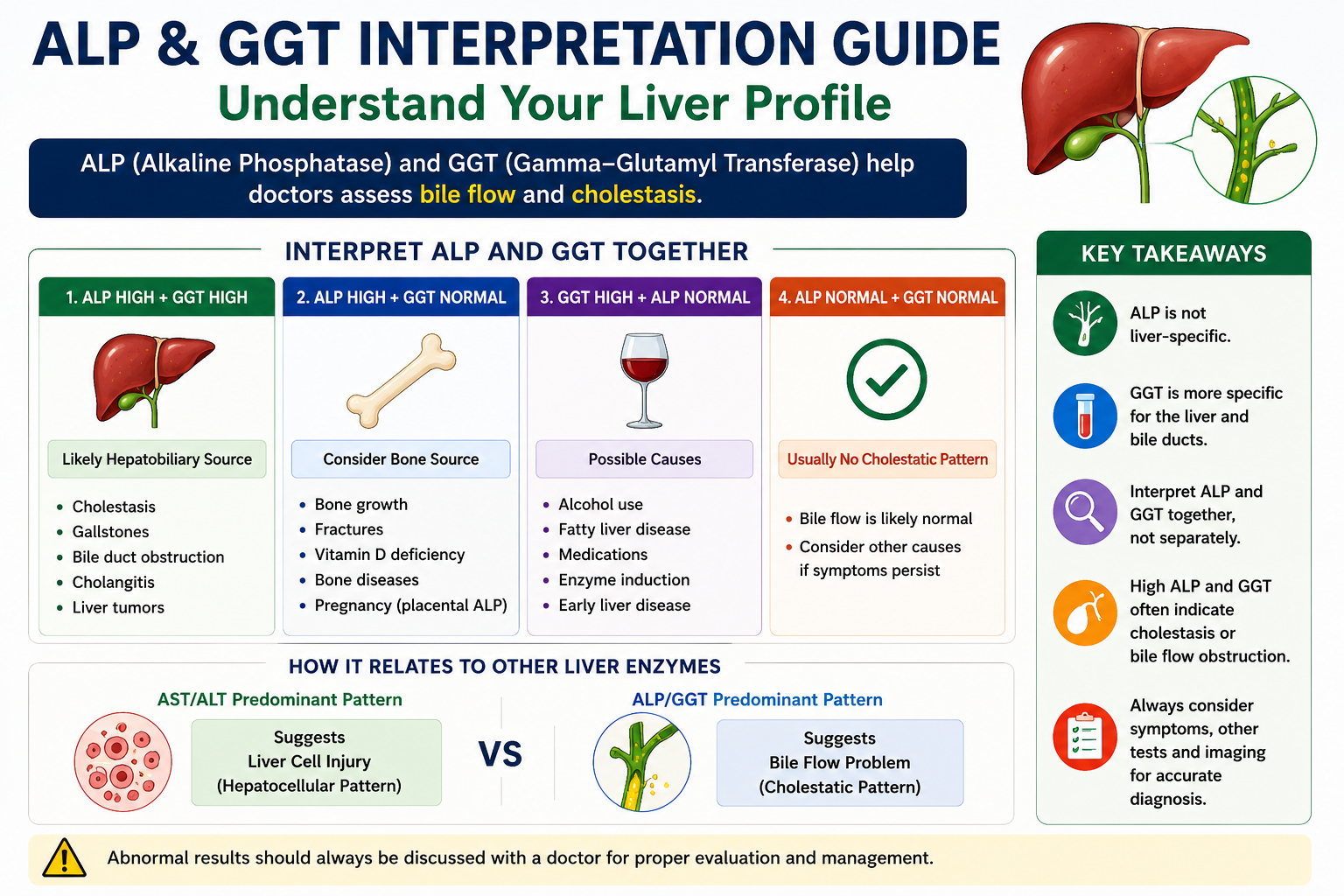
Why are ALP and GGT interpreted together?
Doctors often interpret ALP and GGT together because this combination can help determine whether an abnormal ALP result is likely coming from the liver or from another source such as bone.
This pattern often points toward cholestasis, bile duct obstruction, gallstones or another liver and bile duct problem.
This pattern can occur when ALP is coming from bone, pregnancy or another non-liver source.
Isolated GGT elevation can occur with alcohol use, fatty liver disease, medications or enzyme induction.
The meaning depends on age, pregnancy status, bone health, symptoms and the rest of the report.
| Finding | More suggestive of | Common next step |
|---|---|---|
| ALP high + GGT high | Liver or bile duct source | Review bilirubin and consider ultrasound if clinically indicated |
| ALP high + GGT normal | Bone or other non-liver source | Consider bone profile, vitamin D or other clinical evaluation |
| GGT high + ALP normal | Alcohol, fatty liver, medication effect or enzyme induction | Review history, medicines and other liver tests |
What causes high ALP?
High ALP can come from the liver, bile ducts, bone or other sources. That is why doctors do not interpret ALP alone. They often check GGT and review the rest of the liver profile.
Liver and bile duct causes
- Gallstones
- Bile duct obstruction
- Cholestasis
- Cholangitis
- Liver tumors
- Drug-induced cholestatic liver injury
- Primary biliary cholangitis
- Primary sclerosing cholangitis
Non-liver causes of high ALP
ALP can also rise from non-liver sources because the enzyme is present in bone and several other tissues.
- Bone growth in children and adolescents
- Healing fractures
- Vitamin D deficiency
- Bone disorders
- Pregnancy
- Paget disease
Why ALP may be higher in children and adolescents
Children and adolescents may have higher ALP levels because of active bone growth. This is one reason why an ALP result must be interpreted according to age and clinical context.
Why ALP may be higher in pregnancy
During pregnancy, ALP can rise because the placenta produces ALP. This does not automatically mean liver disease, but symptoms and other test results still matter.
What causes high GGT?
GGT is more closely linked to the liver and biliary system than ALP. It can rise in bile flow problems, liver inflammation, alcohol-related liver disease, fatty liver disease and medication-related enzyme induction.
| Cause | How it may affect GGT |
|---|---|
| Alcohol use | May increase GGT through liver enzyme induction |
| Fatty liver disease | May cause mild to moderate GGT elevation |
| Cholestasis | Often raises GGT together with ALP |
| Medications | Some medicines may increase GGT through liver effects or enzyme induction |
| Hepatitis or liver inflammation | May raise GGT along with other liver enzymes |
Can alcohol increase GGT?
Yes. Alcohol use can increase GGT levels. In some people, GGT may remain elevated even when other liver tests are only mildly abnormal.
Can fatty liver increase GGT?
Yes. Fatty liver disease may cause mild to moderate GGT elevation. This may occur with or without significant bilirubin elevation.
Can medications increase GGT?
Yes. Some medicines can increase GGT through liver enzyme induction or medication-related liver effects. The importance depends on the medicine, dose, duration, symptoms and the rest of the liver profile.
Can ALP be high while GGT is normal?
Yes. When ALP is elevated but GGT remains normal, doctors may consider a non-hepatic source such as bone.
| Possible source | Examples |
|---|---|
| Bone | Growth, fractures, vitamin D deficiency |
| Placenta | Pregnancy |
| Liver | Less likely if GGT remains normal, but clinical context still matters |
Can GGT be high while ALP is normal?
Yes. GGT can be high while ALP remains normal. This is called isolated GGT elevation when other liver profile values are normal or near normal.
Common possibilities include alcohol use, fatty liver disease, medication effects, enzyme induction and metabolic risk factors. In many cases, a mildly high isolated GGT does not automatically mean severe liver disease.
However, it should be interpreted with the patient's history, alcohol intake, medications, body weight, diabetes risk, symptoms and other liver tests.
How do gallstones affect ALP and GGT?
Gallstones can block or intermittently obstruct bile flow. When bile flow is affected, ALP and GGT may rise as part of a cholestatic liver profile pattern.
The pattern can vary depending on whether the obstruction is partial, complete, intermittent or associated with inflammation.
| Situation | Possible liver profile pattern |
|---|---|
| Intermittent obstruction | ALP/GGT may rise and later improve |
| Persistent bile duct obstruction | ALP/GGT and direct bilirubin may rise |
| Gallstone-related inflammation | AST/ALT may also rise, sometimes producing a mixed pattern |
Typical cholestatic pattern with gallstones
| Test | Typical pattern |
|---|---|
| ALP | Elevated |
| GGT | Elevated |
| Direct bilirubin | May increase |
| AST/ALT | May be normal, mildly raised or moderately raised depending on the situation |
When can a bile duct problem become urgent?
A bile duct obstruction can become serious if infection develops. This situation requires urgent medical assessment.
Warning features include:
- Jaundice with fever
- Severe right upper abdominal pain
- Chills or rigors
- Confusion or drowsiness
- Low blood pressure or severe weakness
ALP/GGT versus AST/ALT patterns
Doctors often classify liver profile abnormalities into hepatocellular, cholestatic or mixed patterns.
| Pattern | More suggestive of |
|---|---|
| AST/ALT predominant | Hepatocellular injury |
| ALP/GGT predominant | Cholestatic or bile-flow pattern |
| Mixed pattern | Combined liver injury and cholestasis |
This is the central distinction in liver profile interpretation: AST/ALT points more toward liver cell injury, while ALP/GGT points more toward a bile flow problem. If AST and ALT are high, read more about high AST and ALT results.
Can liver disease exist with normal ALP and GGT?
Yes. Normal ALP and GGT do not completely exclude liver disease. Some liver conditions may mainly affect AST and ALT, while others may have normal blood tests in early stages.
This is why doctors interpret the whole clinical picture, including symptoms, examination findings, risk factors, ultrasound findings and the full liver profile.
What tests may be needed after abnormal ALP or GGT?
The next step depends on whether the pattern looks hepatocellular, cholestatic, mixed or possibly non-liver-related.
| Test | Why it may help |
|---|---|
| Bilirubin | Assess jaundice and bile flow |
| AST and ALT | Assess liver cell injury |
| Albumin and INR | Assess liver synthetic function |
| Ultrasound scan | Assess gallstones and bile ducts |
| Viral hepatitis tests | Assess hepatitis |
| Vitamin D and bone profile | Assess bone-related ALP elevation |
| ALP isoenzymes | May help identify whether ALP is coming from liver, bone or another source in selected cases |
| MRCP or CT | Assess obstruction in selected cases |
The Liver Profile Report Reader can help organize liver profile values before discussing them with a doctor. Protein-related liver profile context is explained in the guide to albumin, globulin and A/G ratio.
When should you see a doctor for high ALP or GGT?
High ALP or GGT should be discussed with a doctor, especially when the abnormality is persistent, rising, clearly above the reference range or associated with symptoms.
- Jaundice
- Dark urine
- Pale stools
- Persistent itching
- Upper abdominal pain
- Fever
- Weight loss
- Persistent vomiting
- Significantly abnormal liver profile
Frequently asked questions about ALP and GGT
Related liver profile guides
ALP and GGT are bile-flow pattern clues
ALP and GGT are important liver profile tests because they help doctors recognize cholestatic or bile-flow patterns. High ALP together with high GGT often points toward a hepatobiliary source, while high ALP with normal GGT may suggest bone or another non-liver source.
The most useful lesson is pattern recognition: AST/ALT mainly suggest a hepatocellular pattern, while ALP/GGT mainly suggest a cholestatic pattern. The final interpretation should always include symptoms, other blood tests and imaging when needed.