Bilirubin results need pattern-based interpretation
Many liver profile reports include bilirubin measurements. Patients commonly ask what bilirubin is, why it is high, whether it means liver disease, and what the difference is between direct and indirect bilirubin.
The answer is often more complex than simply "liver disease." Bilirubin levels can increase due to problems occurring before the liver, within the liver or after the liver. Understanding the pattern helps doctors identify the most likely cause.
What is bilirubin?
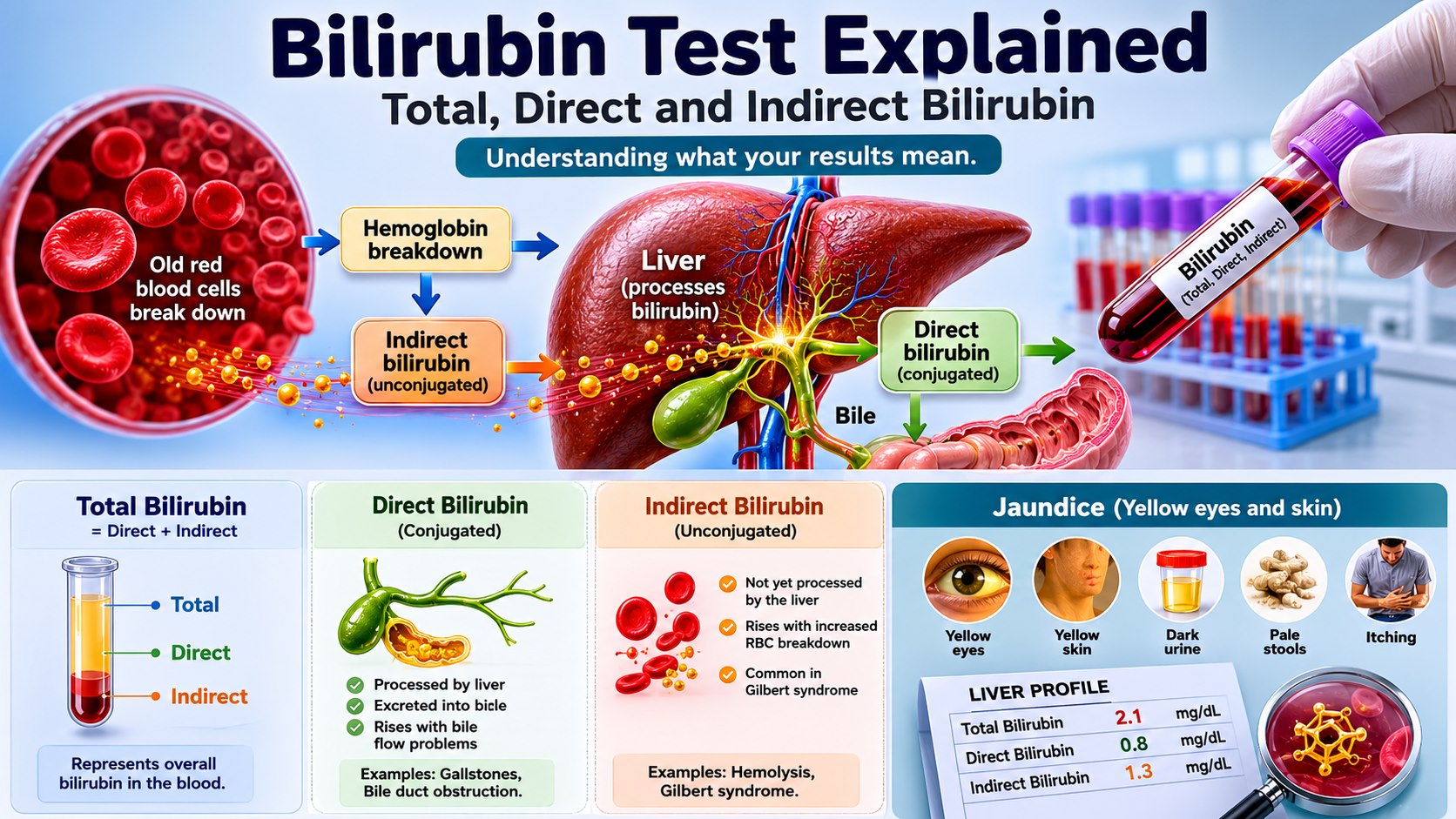
Every day the body removes aging red blood cells and recycles their components. One of the products formed during this process is bilirubin.
Bilirubin is yellow, which is why high bilirubin levels can cause yellow discoloration of the eyes and skin, known as jaundice.
Normal bilirubin ranges
Bilirubin reference ranges can vary slightly between laboratories. Always compare your result with the reference range printed on your own report.
| Test | Common approximate range | Meaning |
|---|---|---|
| Total bilirubin | About 0.2-1.2 mg/dL | The overall amount of bilirubin in blood |
| Direct bilirubin | About 0.0-0.3 mg/dL | Bilirubin already processed by the liver |
| Indirect bilirubin | Usually calculated | Total bilirubin minus direct bilirubin |
How is bilirubin produced?
Bilirubin production follows a step-by-step pathway from old red blood cells to bile and the intestine.
Step 1: Old red blood cells break down
Red blood cells have a limited lifespan. Older cells are removed by the body as part of normal turnover.
Step 2: Hemoglobin is released
Hemoglobin from these red blood cells is broken down and recycled.
Step 3: Indirect bilirubin forms
Indirect bilirubin, also called unconjugated bilirubin, is formed before liver processing.
Step 4: The liver processes bilirubin
The liver takes up indirect bilirubin and changes it into a form that can be excreted into bile.
Step 5: Direct bilirubin forms
Direct bilirubin, also called conjugated bilirubin, is the processed form.
Step 6: Bilirubin enters bile and leaves the body
Direct bilirubin passes into bile, reaches the intestine and is eventually removed from the body.
Why is bilirubin measured?
Doctors may request bilirubin testing during a liver profile, or when symptoms and other results suggest a bilirubin-related problem.
- During a liver profile
- To investigate jaundice
- To assess liver disease
- To evaluate bile duct obstruction
- To investigate hemolysis
- To monitor known liver disorders
Types of bilirubin
Total bilirubin
Total bilirubin represents the overall bilirubin level in the blood. It includes both direct and indirect bilirubin.
Direct bilirubin (conjugated bilirubin)
When bile flow or bilirubin excretion is disrupted, direct bilirubin may accumulate in the bloodstream.
What causes direct bilirubin to rise?
Direct bilirubin commonly rises when processed bilirubin cannot move normally from the liver into bile, or when bile flow is blocked or slowed.
- Gallstones blocking bile flow
- Bile duct obstruction
- Cholestatic liver disease
- Drug-induced cholestasis
- Hepatitis or liver inflammation
- Strictures or narrowing of bile ducts
Indirect bilirubin (unconjugated bilirubin)
Indirect bilirubin is especially useful when doctors are considering conditions such as hemolysis or Gilbert syndrome.
What causes indirect bilirubin to rise?
Indirect bilirubin commonly rises when bilirubin production increases or when the liver has difficulty taking up or processing bilirubin.
- Gilbert syndrome
- Hemolysis, which means increased red blood cell breakdown
- Large bruise or hematoma breakdown
- Fasting or illness in people with Gilbert syndrome
- Some inherited bilirubin-processing conditions
How doctors interpret a bilirubin report
Doctors usually start by looking at the total bilirubin level. Then they check whether the rise is mainly direct bilirubin, mainly indirect bilirubin, or a mixed pattern.
| Example result | Pattern | Possible interpretation |
|---|---|---|
| Total bilirubin 3.0 mg/dL Direct bilirubin 0.2 mg/dL | Predominantly indirect | May suggest Gilbert syndrome or hemolysis, depending on context |
| Total bilirubin 3.0 mg/dL Direct bilirubin 2.2 mg/dL | Predominantly direct | May suggest impaired bile flow, cholestasis or obstruction |
| Total bilirubin 4.0 mg/dL Direct bilirubin 1.8 mg/dL | Mixed elevation | May occur with hepatitis, liver injury or significant liver cell dysfunction |
These examples are for education only. The same number can mean different things in different patients.
Understanding bilirubin patterns
This is the most important part of bilirubin interpretation. Doctors do not look only at whether bilirubin is high. They also look at whether the rise is mainly indirect, mainly direct or mixed.
Predominantly indirect bilirubin elevation
This usually suggests hemolysis, Gilbert syndrome or another pre-hepatic cause. The liver has not yet processed most of the bilirubin.
- Hemolysis
- Gilbert syndrome
- Other pre-hepatic causes
Predominantly direct bilirubin elevation
This usually suggests bile duct obstruction, gallstones, cholestatic liver disease or impaired bile excretion. The liver has already processed bilirubin, but normal excretion is impaired.
- Bile duct obstruction
- Gallstones
- Cholestatic liver disease
- Impaired bile excretion
Mixed bilirubin elevation
A mixed pattern may occur in hepatitis, severe liver injury or significant liver cell dysfunction. Both bilirubin processing and excretion may be affected.
- Hepatitis
- Severe liver injury
- Significant liver cell dysfunction
| Pattern | Common Interpretation |
|---|---|
| Indirect predominance | Pre-hepatic causes, Gilbert syndrome, hemolysis |
| Direct predominance | Obstruction, cholestasis |
| Mixed elevation | Hepatitis, severe liver injury |
Bilirubin pattern summary
| Pattern | Possible clues |
|---|---|
| High indirect bilirubin | Gilbert syndrome, hemolysis or increased bilirubin production |
| High direct bilirubin | Cholestasis, bile duct obstruction or impaired bile excretion |
| Mixed bilirubin elevation | Hepatitis, severe liver injury or liver cell dysfunction |
| High bilirubin with normal AST and ALT | Gilbert syndrome, hemolysis or non-hepatocellular causes |
| High bilirubin with high ALP and GGT | May suggest cholestatic or obstructive pattern |
| High bilirubin with high AST and ALT | May suggest hepatocellular injury or hepatitis pattern |
Common causes of high bilirubin
Gilbert syndrome
Gilbert syndrome is a common inherited condition that can cause mild, intermittent indirect bilirubin elevation. It is often discovered incidentally when a blood test shows raised bilirubin while other liver tests are normal.
In Gilbert syndrome, bilirubin may rise during certain triggers, then return closer to normal later.
| Common trigger | How it may affect bilirubin |
|---|---|
| Fasting or skipped meals | May increase indirect bilirubin temporarily |
| Illness or fever | May trigger a temporary rise |
| Dehydration | May make bilirubin appear higher |
| Physical stress | May contribute to intermittent elevation |
Gallstones
Gallstones can obstruct bile flow. When bile cannot drain normally, direct bilirubin may rise and jaundice may occur.
Hepatitis
Hepatitis means liver inflammation. Depending on severity, a mixed bilirubin pattern may occur because liver processing and excretion can both be affected.
Hemolysis
Hemolysis means accelerated red blood cell breakdown. This increases bilirubin production and commonly raises indirect bilirubin.
Bile duct obstruction
Bile duct obstruction may be caused by stones, tumors or strictures. Direct bilirubin usually rises because processed bilirubin cannot drain normally into bile.
Can bilirubin rise before jaundice appears?
Yes. Bilirubin may become abnormal on a blood test before yellow eyes or yellow skin become obvious.
Jaundice often becomes visible when bilirubin rises to around 2-3 mg/dL, but this can vary between individuals.
What is jaundice?
Jaundice is a visible sign, not a final diagnosis. The cause may be before the liver, within the liver or after the liver.
Common symptoms associated with jaundice
- Yellow eyes
- Yellow skin
- Dark urine
- Pale stools
- Itching
When is jaundice more concerning?
Jaundice should be assessed carefully when it is associated with warning features.
- Dark urine
- Pale or clay-coloured stools
- Severe abdominal pain
- Fever or chills
- Persistent vomiting
- Unexplained weight loss
- Confusion or severe drowsiness
- Bleeding tendency
Can bilirubin be high with normal AST and ALT?
Yes. Bilirubin can be high while AST and ALT are normal. Examples include Gilbert syndrome and hemolysis.
This is an important reason why bilirubin should not be interpreted alone. The pattern, symptoms and other blood tests matter. You can read more about AST and ALT blood tests and high AST and ALT results.
Can AST and ALT be high with normal bilirubin?
Yes. AST and ALT can be high while bilirubin remains normal. Examples include fatty liver, early hepatitis and mild liver injury.
Why ALP and GGT matter when bilirubin is high
ALP and GGT are important when doctors are assessing whether high bilirubin may be related to impaired bile flow.
When direct bilirubin is high together with high ALP and GGT, doctors may consider a cholestatic or obstructive pattern. This can happen when bile flow is blocked or slowed.
| Pattern | Possible direction of interpretation |
|---|---|
| High direct bilirubin + high ALP/GGT | May suggest bile flow obstruction or cholestasis |
| High bilirubin + high AST/ALT | May suggest liver cell injury or hepatitis pattern |
| High bilirubin + normal AST/ALT | May suggest Gilbert syndrome, hemolysis or other non-hepatocellular patterns |
This is why bilirubin should be interpreted together with the complete liver profile, not as an isolated number. Albumin can add another part of the picture; see albumin, globulin and A/G ratio.
Can fasting affect bilirubin levels?
Yes. Fasting may increase bilirubin levels in some individuals, particularly those with Gilbert syndrome. This is usually temporary.
Can dehydration affect bilirubin?
Mild elevations may occasionally occur in dehydration, but interpretation depends on the overall clinical picture.
When should bilirubin testing be repeated?
Repeat testing may be considered when a mild isolated elevation is found, the cause is uncertain or an existing condition needs monitoring. The timing depends on clinical circumstances. For structured context, the Liver Profile Report Reader can help organize liver profile values, and the Liver Scarring Risk Calculator may be useful when liver scarring risk is being assessed.
What tests may be needed after a high bilirubin result?
The next test depends on the bilirubin pattern, symptoms, physical examination and other liver profile results.
| Test | Why it may be useful |
|---|---|
| AST and ALT | Help assess liver cell injury |
| ALP and GGT | Help assess cholestasis or bile flow problems |
| Albumin and INR | Help assess liver synthetic function |
| Full blood count | May help identify anemia, infection or hemolysis clues |
| Reticulocyte count and LDH | May be considered if hemolysis is suspected |
| Viral hepatitis tests | May be needed if hepatitis is suspected |
| Ultrasound scan | May help assess gallstones, bile ducts and liver structure |
When should you see a doctor?
You should discuss high bilirubin results with a doctor, especially if the result is persistent, rising, clearly above the reference range, or associated with symptoms.
- Bilirubin continues to rise on repeat testing
- Yellow eyes or yellow skin develop
- Dark urine occurs
- Pale or clay-coloured stools occur
- Itching becomes persistent
- Significant abdominal pain develops
- Fever or chills occur with jaundice
- Unexplained weight loss occurs
- Persistent vomiting occurs
- Other liver profile results are also abnormal
Frequently asked questions about bilirubin
Related liver profile guides
Bilirubin interpretation depends on the pattern
Bilirubin is formed when old red blood cells break down, then processed by the liver and excreted into bile. Total bilirubin tells you the overall level, while direct and indirect bilirubin help identify where the problem may be occurring.
A high bilirubin result should be interpreted with symptoms, examination findings, AST, ALT, ALP, GGT, blood counts and imaging when needed. The pattern matters more than one number alone.