What is the HbA1c Test?
The HbA1c test (Glycated Haemoglobin test) measures the percentage of haemoglobin in your red blood cells that has glucose attached to it. When glucose circulates in your blood, a portion of it naturally binds to haemoglobin — the protein that carries oxygen inside red blood cells. The higher your blood sugar has been over time, the more haemoglobin becomes glycated.
Because red blood cells live for approximately 2–3 months, the HbA1c result reflects your average blood sugar level over that entire period — not just at a single moment in time. This makes it far more informative than a random or fasting blood glucose test for understanding long-term sugar control.
Why is HbA1c Important?
HbA1c is one of the most widely used tests in diabetes care. It serves two major roles: diagnosing diabetes and prediabetes, and monitoring long-term blood sugar control in people already living with diabetes.
Key Advantages Over Other Tests
When Should You Do an HbA1c Test?
For Diagnosis — Who Should Be Tested?
HbA1c is especially useful for screening and diagnosing diabetes and prediabetes in the following groups:
- 1Overweight or obese individuals — particularly if BMI is 25 or above (or lower cut-offs in South Asians)
- 2Strong family history of diabetes — especially first-degree relatives (parents, siblings) diagnosed before age 50, or multiple affected family members
- 3Hypertension (high blood pressure) or other features of metabolic syndrome
- 4Routine screening in adults aged 35–40 and above in Sri Lanka, where Type 2 diabetes is increasingly prevalent at younger ages
What Counts as a "Strong" Family History?
Not all relatives with diabetes convey the same level of inherited risk. The following situations are considered more significant:
For Monitoring — Patients Already Diagnosed with Diabetes
How is the HbA1c Test Done?
The HbA1c test is one of the most straightforward blood tests available. There is no preparation required beyond arriving at the laboratory.
- 1A small blood sample is taken — usually from a vein in your arm, exactly like any other routine blood test.
- 2No fasting needed — you can eat, drink, and take your medications as normal before the test.
- 3No glucose drink required — unlike the OGTT, there is nothing to drink and no waiting period in the laboratory.
- 4Result is returned as a percentage — for example, 7.2%, which your doctor interprets against standard reference ranges.
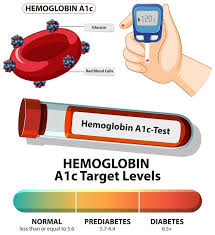
HbA1c Reference Values & Interpretation
The table below shows the standard diagnostic thresholds used internationally and in Sri Lanka.
| Category | HbA1c (%) | Interpretation |
|---|---|---|
| Normal | < 5.7% | Normal |
| Prediabetes | 5.7% – 6.4% | At Risk — Prediabetes |
| Diabetes | ≥ 6.5% | Diabetes |
Treatment Targets for Patients Already Diagnosed with Diabetes
Once diabetes is diagnosed, the HbA1c target depends on the individual. Your doctor will set a personalised target based on your age, other health conditions, and the risk of hypoglycaemia. General guidelines are:
| Control Level | HbA1c Target | Status |
|---|---|---|
| Good control | < 7% | Well Controlled |
| Moderate control | 7% – 8% | Needs Attention |
| Poor control | > 8% | Review Treatment |
What Do Abnormal Results Mean?
When HbA1c May Be Unreliable
HbA1c is a very useful test, but it is not perfect. Because it depends on haemoglobin inside red blood cells, any condition that changes red blood cell lifespan or haemoglobin structure can produce a misleading result.
-
Anaemia (especially iron-deficiency anaemia) — iron deficiency causes red blood cells to live longer, increasing glucose exposure time and falsely raising the HbA1c result.
-
Recent blood transfusion — transfused red blood cells have not been exposed to your blood sugar levels, falsely lowering the result.
-
Chronic kidney disease (CKD) — kidney disease causes anaemia and shortens red blood cell survival, affecting the result.
-
Haemoglobin disorders — sickle cell disease, thalassaemia, and other haemoglobin variants affect how the test measures glycation, potentially producing an inaccurate reading.
HbA1c vs OGTT — Which Test is Better?
HbA1c and the OGTT each have distinct strengths. They are not interchangeable in every situation — the right test depends on your clinical circumstances.
| Feature | HbA1c | OGTT |
|---|---|---|
| Fasting required | No | Yes (8–12 hours) |
| Time taken | A few minutes | 2–3 hours |
| Detects early (borderline) diabetes | Less sensitive | More sensitive |
| Preferred in pregnancy | Not recommended | Gold standard (GDM) |
| Reliable with anaemia or haemoglobin disorders | No | Yes |
| Reflects long-term control | Yes (2–3 months) | No (single time point) |
| Widely used in Sri Lanka for monitoring | Yes | No (mainly diagnostic) |
• HbA1c → widely used for routine screening, diagnosis in stable patients, and ongoing monitoring
• OGTT → essential in pregnancy for diagnosing gestational diabetes (GDM); also preferred when HbA1c may be unreliable
The two tests are often complementary — a borderline HbA1c result may warrant an OGTT for confirmation, particularly in younger patients or when early diabetes needs to be excluded with higher confidence.
Common Mistakes — and How to Avoid Them
-
Ignoring known anaemia — if you have iron-deficiency anaemia or any blood disorder, tell your doctor before relying on HbA1c results. A falsely elevated HbA1c in an anaemic patient can lead to unnecessary treatment.
-
Testing during acute illness — acute illness or recent surgery can temporarily affect blood sugar levels. HbA1c is less affected than random glucose, but testing during an acute event is still not ideal for making long-term management decisions.
-
Assuming one normal result is enough forever — HbA1c should be repeated at intervals appropriate to your risk. A normal HbA1c today does not provide lifelong reassurance — especially if you have ongoing risk factors such as obesity or a strong family history.
-
Misinterpreting "borderline" values — an HbA1c of 6.0% or 6.1% is not diabetes, but it is prediabetes and requires action. Dismissing a borderline result as "almost normal" misses the opportunity for preventive intervention.
-
Stopping medications before the test — some patients stop their diabetes medications hoping to "reset" their result. This does not help — HbA1c reflects the last 2–3 months, so omitting medication for a few days before the test makes no meaningful difference to the result but can be harmful to your blood sugar control.
Frequently Asked Questions
- Every 3 months — if your diabetes is poorly controlled or you have recently changed your treatment
- Every 6 months — if your blood sugar is stable and well controlled
- HbA1c measures your average blood sugar over the past 2–3 months — not just at one moment in time
- No fasting required — it can be done at any time of day
- Normal: below 5.7% | Prediabetes: 5.7%–6.4% | Diabetes: 6.5% or above
- Treatment target for most diabetic patients: below 7% — personalised by your doctor
- Not recommended for diagnosing gestational diabetes in pregnancy — OGTT is preferred
- May be unreliable in anaemia, recent blood transfusion, kidney disease, or haemoglobin disorders
- For ongoing diabetes management, always interpret HbA1c alongside your doctor's clinical assessment
